Novel Use of a Shock Wave Device for Energy Flux Density Threshold Testing of the Distal Ventral Erect Penile Shaft as a Marker of Penile Dysesthesia/Hypersensitivity Associated with Premature Ejaculation
(Uloko et al., 2020. 21st Annual Fall Scientific Meeting of Sexual Medicine Society of North America (SMSNA), Abstract No.041)
San Diego Sexual Medicine
Introduction: Premature ejaculation (PE) is the most common sexual dysfunction in men. Traditional PE management is based on pharmacologic strategies to increase/decrease central inhibition/excitation, respectively. A subset of PE patients was identified with extreme penile hypersensitivity; simply touching the frenular region during sexual activity resulted inevitably in premature ejaculation. The clinical dilemma is that there are no objective and clinically relevant clinical tests of penile dysesthesia/hypersensitivity to successfully identify this subset of PE patients
Objectives: We herein describe, in a subset of men with PE, a novel biologic marker for penile dysesthesia/hypersensitivity.
Methods: Energy flux density is a measure of the energy per square area (mJ/mm2) released by a shockwave pulse at a specific location. The threshold of energy flux density tolerable to the patient was determined during pharmacologic penile erection. The UroGold 100 MTS OP155 parabolic probe, Hz 3 was applied to the right and left lateral mid-shaft, the dorsal mid-shaft, the proximal ventral shaft and the distal ventral shaft overlying the frenulum. At each location, the patient was asked if there was pain on a 4-point scale (0 none, 1 mild, 2 moderate, 3 severe). We started with energy flux density values of 0.05 mJ/mm2 and increased to a maximum of 0.14 mJ/mm2, if tolerable. Energy flux density threshold was defined as the energy flux density when the patient experienced a 2-3 pain level. In those who demonstrated peri-frenular penile dysesthesia/hypersensitivity, the extent of the dysesthesia was mapped, the region was numbed (penile anesthesia test) and the patient was asked to masturbate in a private setting, usually in the office, to determine ejaculation latency.
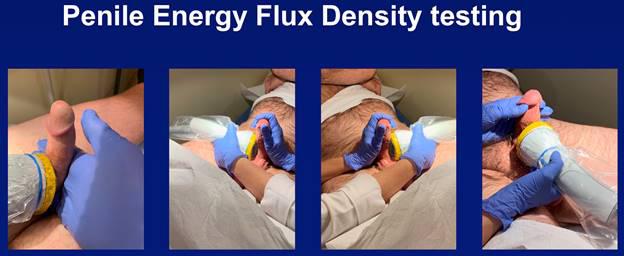
Results: 51 men without PE (mean age 48 +/- 15, IELT > 5 min) and 14 men with PE (IELT < 1 min) (mean age 25 +/- 7) were studied during pharmacologic penile erection. In men without PE, the energy flux density threshold in all erect penile locations was 0.12 – 0.14 mJ/mm2. In the 14 men with PE, the energy flux density threshold in the distal erect ventral shaft region was significantly lower at 0.05 – 0.07 mJ/mm2, while all other erect penile locations yielded threshold values similar to men without PE (0.12 – 0.14 mJ/mm2). 9 patients underwent penile anesthesia testing and IELT values during masturbation increased to over 10 minutes. Figure 1 depicts the novel use of erect penile shockwave energy flux density testing as a diagnostic marker in this subset of men with PE.
Conclusion: Energy flux density threshold may be the first objective, sensitive, clinically relevant biologic marker to identify men whose PE is a result of a localized penile dysesthesia/hypersensitivity in the peri-frenular region. Identification of this subset of PE patients could lead to alternative strategies to cure their PE.